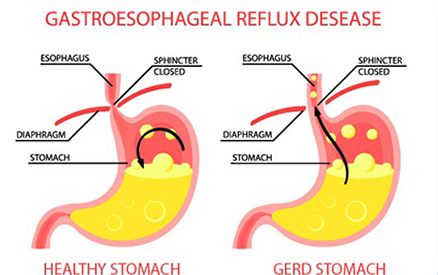
Gastroesophageal reflux disease (GERD) is a common gastrointestinal condition occurring due to the retrograde flow of refluxate from the stomach into the esophagus. The most typical symptoms in GERD are regurgitation and heartburn. Gastro-esophageal refluxate contains a variety of noxious agents, mainly acid but also pancreatic enzymes, pepsin and bile salts. Exposure of the esophageal mucosa to these agents may result in critical injuries to the delicate structures, resulting in reflux esophagitis, esophageal stricture, Barrett’s esophagus, esophageal adenocarcinoma and others.
Even though GERD is a very common clinical diagnosis, its pathogenesis is quite complicated. In many cases, this is due to inappropriate lower esophageal sphincter (LES) function. The pathogenesis of GERD involves an interplay of neurological, chemical, mechanical and psychological mechanisms, which contribute to symptom presentation and influence diagnosis and treatment. Owing to the multifactorial development, many patients may continue to experience detrimental symptoms due to GERD, despite prolonged acid suppression with proton pump inhibitor therapy.1
Pharmacotherapy for GERD
Treatment of GERD is broadly targeted at providing symptomatic relief and preventing the onset of complications such as esophagitis or adenocarcinomas. Treatments take a multifactorial approach that includes lifestyle modifications, medical management with antacids, antisecretory agents, and other pharmacotherapeutic options. Occasionally, surgery may be advised in refractory cases.
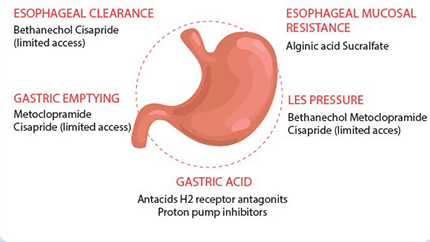
The commonly prescribed pharmacotherapeutic agents include -
1) PPIs (Proton Pump Inhibitors)
Proton pump inhibitors (PPIs) are first choice treatment in GERD. Standard PPI therapy is effective in 90%–100% of people with mild symptoms; however, effectiveness decreases to 60% in people with the most severe disease.2Evidence indicates that for maintenance therapy, low-dose PPI is as effective as high dose.3 However, despite their efficacy, about 20–30% of patients report an insufficient response and alternative drugs are required.4
2) Prokinetic drugs
Prokinetic drugs can be useful adjuncts in the treatment of GERD by increasing the LES pressure, enhancing gastric emptying, or improving peristalsis. Clinically, however, these drugs are marginally useful.
3) Mucosal protective drugs
Mucosal protective agents are inferior to antacid/ alginates, H2RAs and PPIs in the treatment of erosive esophagitis and in relieving symptoms of GERD. They have limited usefulness in the treatment of duodenal and gastric ulcers.
4) Histamine and H2 Receptor Antagonists
H2RAs are safe and effective in controlling symptoms of acute reflux disease. It is important that patients visit their physician before using H2RA medications beyond their 14-day indication.5
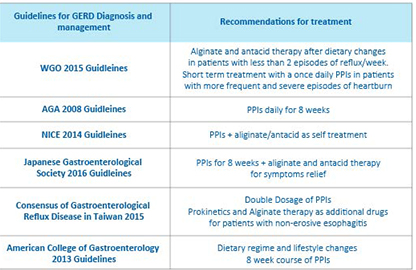
Guideline Recommendations for GERD Management
Although PPIs stay the first choice for treatment of GERD, often other drugs are prescribed as an adjunct for different variants of GERD (based on duration and symptoms), which can not be treated by PPIs alone. Different
guidelines suggest monotherapy or a combination of one or more of these medications to treat GERD.6
The Need For Alginate-Based Therapy in GERD
Alginate-based formulations act primarily by a unique nonsystemic mechanism of action, different from antacids, PPIs or histamine H2-receptor antagonists (H2 antagonists). Upon coming into contact with gastric acid, alginate rapidly forms a gel ‘raft’ of near-neutral pH that creates a protective barrier above the acidic gastric contents. This alginate raft protects the oesophageal mucosa by limiting gastric reflux into the oesophagus.7
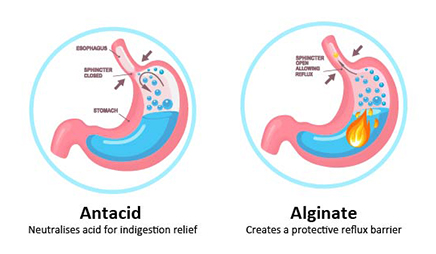
Alginate-based formulations have been shown to act more rapidly than PPIs and H2 antagonists,8 and to provide longer-lasting relief of symptoms than conventional antacids. These formulations have been shown to provide effective relief of upper gastrointestinal (GI) symptoms, either as a monotherapy or in combination treatment. These findings suggest that alginate-based formulations could be considered as an alternative or add-on therapy in GERD patients, including those with non-erosive reflux disease or NERD.9
Alginate Therapy is Clinically Established in GERD
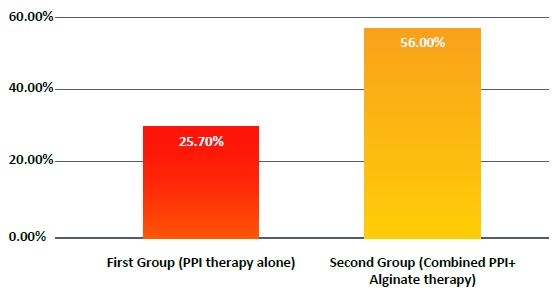
Manabe et al. investigated the benefit of adding alginate to antacid therapy in patients with NERD. The authors conducted a randomized, open-label, parallel group multicenter study, including 76 patients, randomly assigned into two groups, receiving either alginate and antacid, or antacid alone. They reported that 56% of patients from the first group presented resolution of symptoms compared to only 25.7% of the ones from the second group, and concluded that combined PPI and alginate therapy was superior to PPI therapy alone.10
Several other studies have found therapeutic benefits of alginates in GERD
• An immediate therapeutic action with alginate (within 1h of administration) was observed, which was considered faster in comparison to a PPI or an H2-receptor antagonist (H2RA).11
• Alginate was found superior to placebo and antacids for the treatment of mild GERD, and this monotherapy seems to be beneficial as an initial treatment.12 In the sodium alginate group, symptom resolution was observed to be higher, and the speed of action was faster in comparison to the antacid group.
• Alginates were also shown to be effective for self-medication to control mild reflux disease.13
• In the most recent randomized clinical trial, an alginate-containing product has been shown to be superior to antacid in post-supper suppression of the acid pocket in obese individuals.14
• Alginate-based therapies were found to be more effective in treating GERD symptoms as compared with placebo or antacids.15
Alginates provide effective and immediate relief of reflux symptoms. Owing to their unique mechanism of action and faster relief, alginate-based treatment for GERD can be an effective adjunct to standard treatment with antacids alone.
References:
1.Moshkowitz, Menachem et al. “Gastroesophageal reflux disease symptoms: prevalence, sociodemographics and treatment patterns in the adult Israeli population.” World journal of gastroenterology vol. 17,10 (2011): 1332-5. doi:10.3748/wjg.v17.i10.1332
2. Iwakiri K. Treatment strategy for standard-dose proton pump inhibitor-resistant reflux esophagitis. J Nippon Med Sch. 2017;84(5):209–214
3. (2) 4 Savarino, E., Zentilin, P., Marabotto, E., Bodini, G., Della Coletta, M., Frazzoni, M., ... & Savarino, V. (2017). A review of pharmacotherapy for treating gastroesophageal reflux disease (GERD). Expert opinion on pharmacotherapy, 18(13), 1333-1343.
5. Nguyen L, Birk J. Current and Prospective Pharmacotherapies in Gastroesophageal Reflux Disease. Clinical Medicine Therapeutics. January 2009. doi:10.4137/CMT.S2744
6. Chapelle, Nicolas, et al. "The pharmacotherapeutic management of gastroesophageal reflux disease (GERD)." Expert opinion on pharmacotherapy 22.2 (2021): 219-227.
7. Yu-Min Kung, Wen-Hung Hsu, Meng-Chieh Wu, Jiunn-Wei Wang, Chung-Jung Liu, Yu- Chung Su, Chao-Hung Kuo, Fu-Chen Kuo, Deng-Chyang Wu, Yao-Kuang Wang,Recent Advances in the Pharmacological Management of Gastroesophageal Reflux Disease, Digestive Diseases and Sciences,10.1007/s10620-017-4830-5, 62, 12, (3298-3316), (2017).
8. C. Coyle, G. Crawford, J. Wilkinson, S. J. Thomas, P. Bytzer, Randomised clinical trial: addition of alginate‐antacid (Gaviscon Double Action) to proton pump inhibitor therapy in patients with breakthrough symptoms, Alimentary Pharmacology & Therapeutics. 10.1111/apt.14064, 45, 12, (1524-1533), (2017).
9. C. Coyle, P. Bytzer, Editorial: refractory GERD—good drug, wrong patients? Authors’ reply, Alimentary Pharmacology & Therapeutics, 10.1111/apt.14151, 46, 2, (204-205),(2017).
10. Manabe, N., et al. "Efficacy of adding sodium alginate to omeprazole in patients with nonerosive reflux disease: a randomized clinical trial."Diseases of the Esophagus 25.5 (2012): 373-380.
11. Dettmar PW, Sykes J, Little SL, Bryan J. Rapid onset of effect of sodium alginate on gastro-oesophageal reflux compared with ranitidine and omeprazole, and relationship between symptoms and reflux episodes. Int. J. Clin. Pract. 2006; 60: 275– 83.
12. Bor S, Kalkan IH, Celebi A et al. Alginates: from the ocean to gastroesophageal reflux disease treatment. Turk. J. Gastroenterol. 2019; 30(Suppl. 2): 109– 36.
13. Tytgat GN. Review article: treatment of mild and severe cases of GERD. Aliment. Pharmacol. Ther. 2002; 16 (Suppl. 4): 73– 8.
14. Deraman MA, Abdul Hafidz MI, Lawenko RM et al. Randomised clinical trial: the effectiveness of Gaviscon Advance vs non-alginate antacid in suppression of acid pocket and post-prandial reflux in obese individuals after late-night supper. Aliment. Pharmacol. Ther. 2020; 51: 1014– 21
15. Leiman DA, Riff BP, Morgan S et al. Alginate therapy is effective treatment for GERD symptoms: a systematic review and meta-analysis. Dis. Esophagus. 2017; 30: 1– 9