Osteoarthritis (OA) and Inflammatory Arthritis (IA) are two common chronic, degenerative disorders. They have a huge impact on daily self-care and the quality of life of the patients. In both OA and IA, pain is the most prominent symptom. Pain is a multifactorial process that may cause tissue damage, disability, and psychological concerns. The major aim of pain management includes improved functions, increased well-being, and reduced individual and societal costs. Inflammatory arthritis affects over 180 million people in India, more than many well-known diseases like diabetes, AIDS, and cancer. Osteoarthritis affects 15 million adults annually, with the prevalence ranging between 22 to 39% in India. This condition is more common in women than in men, and the prevalence increases with age.1
The EULAR Committee
The aim of the EULAR guidelines was to,
• Evaluate all the scientific evidence and expert opinion on pain management in IA and OA.
• Develop evidence-based recommendations for health professionals in the field of rheumatology to offer pain management support for people with IA and/or OA.
• 18-member task force from 12 countries, including the USA.
• The team consisted of patient-representatives, nurses, physiotherapists, rheumatologists, general practitioners, psychologists, clinical epidemiologists, occupational therapists and a research fellow.
A Step-by-step approach by the EULAR task force
1. A thorough search of 2914 selected titles was conducted. Out of this, 186 systematic reviews and meta-analyses were included to assess the population, types of interventions, effects, and the level of quality.
2. The task force then developed their recommendations based on discussions of the literature review results.
3. Post discussion; the recommendation wordings were finalized and shared through email, with the task force members indicating their level of agreement for each of the recommendations.
The task force developed four overarching principles for rheumatologists and other physicians founded on expert opinion.
• The process of assessment and treatment should be led by patient-centric agenda.
• The health professional should take into consideration the fact that pain encompasses multiple and mutually interacting biological, psychological and social factors that include but are not limited to
pain severity, inflammation and joint damage, central neurophysiological processes, physical ability, resilience and emotional vulnerabilities, social factors, sleep quality, obesity and other health risks such as smoking and alcoholism.
• The basic knowledge of the pathology, treatment and the after effects of the condition and treatment of IA and OA should be known to the health professional.
• The health professional should be able to recognize between localized and generalized pain and should be mindful that these types of pain may even coexist.
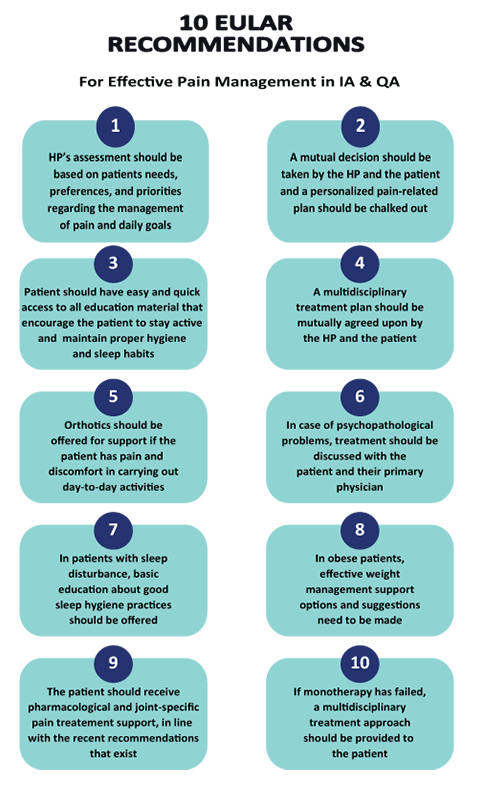
1. The assessment by the health professional (HP) should be based on the patient’s needs, preferences, and priorities regarding the management of pain and goals in daily life. It should be based on the pain severity, types, spread, quality, and other characteristics. The HP should also assess the current inflammation and joint damage as sources of pain and whether or not they have been adequately treated. Also, pain-related factors such as disability, beliefs, and emotions regarding pain-related disability, social influences related to pain, sleep, and obesity need to be looked into.
2. A personalized pain management plan should be provided that aims at reducing pain-related distress and improving pain-related functions in daily life. The plan should be a product of the outcome of shared decision-making between the HP and the patient.
3. All patients should have easy and quick access to the education materials such as brochures, links to online resources, etc., that encourage the patients to stay active, maintain appropriate sleep hygiene, and more. The patients should have access to psychoeducation by the HP’s and online or in-person, face-to-face self-management interventions.
4. The HP and the patient should mutually decide whether advice to stay active, supervised physical exercise, or multidisciplinary treatment is required. If the patient is unable to initiate physical activity without help, a referral to a physiotherapist for personalized physical exercise or strength training should be arranged. A multidisciplinary intervention such as cognitive-behavioural therapy (CBT) should be considered if psychosocial factors such as fear of movement or catastrophizing cognition underlie a
disabled, sedentary lifestyle of a patient.
5. If the patient has pain and discomfort in carrying out daily activities that affect their functioning, orthotics such as braces, splints, insoles, special shoes, etc., daily living aids, assistive devices such as canes, and other ergonomic devices should be offered for support. An occupational therapist should be considered if the patient wants to use assistive support.
6. Basic social and psychological management support or referral to a psychologist, social worker, self-management support program, CBT, or multidisciplinary treatment should be provided if social or psychological factors interfere with effective pain management and functional status. If the patient is suffering from psychopathological problems such as depression or anxiety, treatment options should be discussed with the patient and the patient’s primary care physician.
7. In case of sleep disturbance in the patients, upon inquiry of causes, basic education about good sleep hygiene practices should be offered. If the problem of sleep persists, referral to a therapist or a program aimed at sleep restoration or a specialized sleep clinic should be made.
8. In obese patients, the link between obesity and its contribution to pain and disability should be discussed. The patient should be provided with effective weight management options, and suggestions should be made regarding specialized weight management support such as a referral to a dietician, a
psychologist, or a bariatric clinic.
9. Upon investigating the patient’s existing use of prescribed medications, over-the-counter pain relief medications, homeopathic remedies, and the frequency of use, the patient should receive pharmacological and joint-specific pain treatment support, in line with the recent recommendations that exist.
10. If monotherapy has failed, a multidisciplinary treatment approach should be provided to the patient.
Chronic pain is one of the most common complaints affecting people with inflammatory arthritis and osteoarthritis. Of the many treatment options available, the European League against Rheumatism (EULAR) has provided recommendations that serve as a great resource for the HP’s to have on hand while treating patients with IA and OA.2
References:
1. Pal, C., Singh, P., Chaturvedi, S., Pruthi, K. and Vij, A., 2016. Epidemiology of knee osteoarthritis in India and related factors. Indian Journal of Orthopaedics, 50(5), p.518.C
2. Geenen, R., Overman, C., Christensen, R., Åsenlöf, P., Capela, S., Huisinga, K., Husebø, M., Köke, A., Paskins, Z., Pitsillidou, I., Savel, C., Austin, J., Hassett, A., Severijns, G., Stoffer-Marx, M., Vlaeyen, J., Fernández-de-las-Peñas, C., Ryan, S. and Bergman, S., 2018. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Annals of the Rheumatic Diseases, pp.annrheumdis-2017-212662.